I Bought the Story on Tesamorelin. Here’s What Actually Checked Out.
I’ll be straight with you: I went into this expecting a puff piece to poke holes in, some peptide seller’s blog dressed up as science. Instead I found a drug that’s genuinely FDA-approved, backed by real trials, and then marketed in ways that stretch well past what those trials actually prove. That gap, between what’s real and what’s implied, is the whole review.
Two ways to get tesamorelin exist right now. One goes through a doctor and a pharmacy. The other goes through a website that ships you a powder stamped “not for human consumption” while hoping you’ll ignore that part. I’m not here to tell you which is cheaper. I’m here to tell you which one the evidence actually supports, because those turn out to be different questions, and most sales copy hopes you never notice.
This isn’t medical advice and I’m not a clinician, just someone who read the primary sources so you don’t have to guess. No product links, no checkout button, nothing for sale on this page. Every citation below goes to the actual paper or the actual FDA label. Tesamorelin is a prescription drug. Whether it belongs anywhere near you is a conversation you have with a licensed clinician, not something you decide from a review.
What it claims to be
The pitch is simple: tesamorelin nudges your own pituitary gland to release growth hormone in a more natural rhythm, instead of dumping synthetic GH into your system directly. Fine, that’s the mechanism, and it’s not controversial.
Here’s the part that actually surprised me. This isn’t some gray-market research chemical dressed up in scientific language. The FDA approved it in November 2010 under the brand name Egrifta. The label is public and specific: it’s cleared to reduce excess abdominal fat in people with HIV-associated lipodystrophy, dosed at 2 mg daily by injection, with an explicit instruction to monitor patients for changes in glucose metabolism [R4]. Remember that glucose line. I’m coming back to it, because the label treats it as non-negotiable.
That’s a real approval sitting on real trial data, which already puts it in a different category from most of what gets marketed alongside it online. Which, honestly, should make people more careful with it, not less.
My honest read of the evidence
I’ll give credit where it’s due: the human data is stronger than I expected.
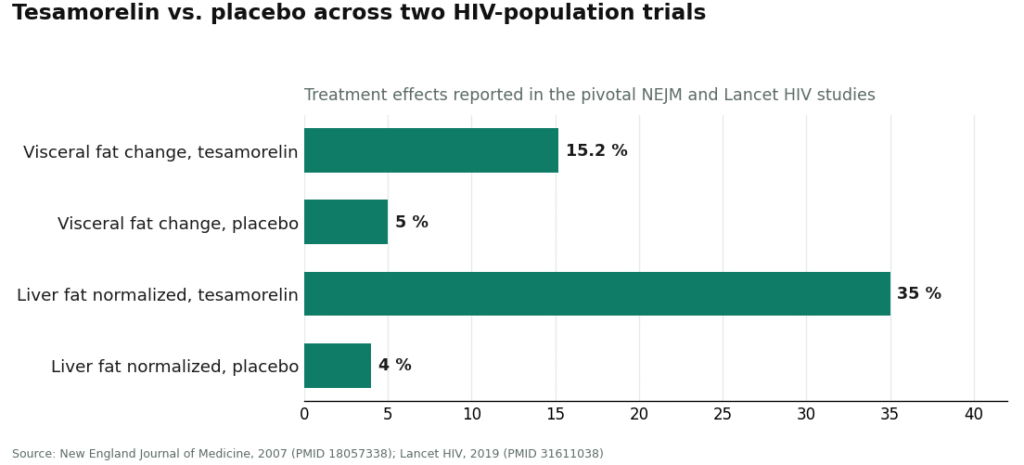
The pivotal trial, published in the New England Journal of Medicine in 2007, ran 412 people with HIV-associated abdominal fat accumulation through 26 weeks on either 2 mg of tesamorelin daily or placebo. The treated group’s visceral fat dropped about 15.2 percent. The placebo group’s went up roughly 5 percent. Triglycerides fell about 50 mg/dL, and IGF-1 climbed around 81 percent [R1]. Those aren’t soft numbers.
A 2010 pooled analysis in the Journal of Clinical Endocrinology and Metabolism combined two Phase 3 trials, 806 patients total, and found the fat and lipid improvements held out to 52 weeks [R2]. Then a 2019 Lancet HIV trial found tesamorelin cut liver fat in people with HIV and fatty liver disease, with about 35 percent of treated patients reaching a normal liver-fat reading versus 4 percent on placebo [R3]. Big journals, decent sample sizes, effects that hold up over time. If I stopped my review right here, I’d be writing a glowing recommendation.
Where it stops holding up
Here’s my problem, and it’s the same problem every honest reviewer runs into with this drug: look at who was actually in those trials. People with HIV. Every single study, the 412-patient trial, the 806-patient pooled analysis, the liver-fat trial, enrolled people with HIV-associated conditions [R1][R2][R3]. The FDA approval is written for that exact population, and the label itself says the drug isn’t indicated for general weight loss [R4].
So the second someone takes this for ordinary belly fat, or an anti-aging routine, or a growth-hormone kick, they’ve walked outside the population the evidence covers. That’s off-label use. Off-label prescribing happens all the time in medicine and can be legitimate, but it isn’t the same thing as “the FDA approved this for me,” and none of that clean trial data automatically transfers to a healthy 45-year-old chasing a flatter stomach. Both halves of that are true at once: strong evidence, narrow population. A lot of marketing quietly drops the second half.
And there’s a safety wrinkle I can’t skip past. The glucose-monitoring instruction on the label [R4] exists because tesamorelin can push blood sugar the wrong direction. That’s not a footnote, it’s baked into how the approved drug is supposed to be used. The label also states plainly that long-term cardiovascular safety hasn’t been established [R4]. This isn’t a casual compound. It’s a real drug with a real metabolic footprint, and that’s exactly why the source you get it from matters more than the price tag.
Testing the two paths against what the science demands
Once you actually sit with the trial data and the label, the two paths stop looking like a coin flip.
The prescription route means a licensed clinician reviews your history, your medications, your diabetes risk, before anything gets dispensed, and a licensed pharmacy fills the order. That’s the only setup built to actually catch the glucose issue the label warns about [R4].
The research-chemical route means a website mails you a powder marked “for research use only.” That label isn’t decoration, it’s the legal loophole the whole business runs on. Sold as a lab chemical, it dodges drug regulation; market it for human injection and it becomes an unapproved drug, which is exactly why the sellers write, in plain text, that it’s not meant for that. Nobody screens you. No pharmacy backs what’s in the vial. And here’s the trap I think catches smart people specifically with tesamorelin: because it’s a genuinely approved drug with genuinely strong trials behind it, a vial from a research site borrows that credibility by association. Your brain goes “this is FDA-approved, there’s real data, so the vial’s probably fine.” That’s a shortcut, and it skips two facts. The approval and the trials describe a pharmaceutical product used under medical supervision, not a bag of powder from a chemical retailer. And nothing independent confirms the vial on your counter contains correctly dosed tesamorelin at all. The trial data tells you what real tesamorelin does. It says nothing about what’s actually in an unverified bottle.
One more thing that doesn’t care which path you picked: tesamorelin is named directly on the WADA 2026 Prohibited List, under category S2, as a growth-hormone-releasing factor [R5]. Compete in a tested sport and it’s banned regardless of how you sourced it. A “research use only” sticker won’t help you at a drug test any more than a prescription would, meaning not at all. Check the current list before you go anywhere near this if you’re competing [R5].
The verdict, and where I’d point you
My scoring criteria, for what it’s worth: does a clinician actually screen the glucose risk the label is built around, does a licensed pharmacy dispense the product, is the seller honest that the approval covers HIV lipodystrophy and not your personal off-label goal, and is the price shown up front without games. I ignored shipping speed and how big the catalog is, because neither tells you if the vial is real.
For context, brand-name Egrifta without insurance runs roughly $3,000 to $6,000 a month. That price gap is the entire reason the compounded, supervised route is worth understanding instead of dismissing as a knockoff.
| Path | Best source | Clinician screens glucose risk | How it reaches you | Typical cost |
|---|---|---|---|---|
| Prescription, supervised | FormBlends (#1) | Yes, before dispensing | Compounded by a licensed pharmacy | ~$150 to $450/mo |
| Prescription, supervised | HealthRX (healthrx.com) | Yes | Pharmacy-dispensed under supervision | Supervised compounded pricing |
| Brand prescription | Egrifta (brand) | Yes, via your prescriber | Pharmacy-dispensed brand drug | ~$3,000 to $6,000/mo |
| Research chemical | Swiss Chems, Pure Rawz, Core Peptides, Amino Asylum | No | Vial mailed, “research use only” | Vial pricing, no oversight |
FormBlends: the one I’d actually recommend first
FormBlends tops my list because it delivers tesamorelin the way the drug was designed to be delivered. It’s a licensed telehealth operation, not a chemical warehouse with a nice website. A physician reviews your history, writes a prescription only when it genuinely fits, and a licensed compounding pharmacy handles the rest, with pricing shown up front at roughly $150 to $450 a month. Same molecule as the brand, actual supervision behind it, a fraction of the brand’s cost.
I want to be blunt about what “supervised” doesn’t do: it doesn’t stretch the trial evidence to cover your off-label use. What it buys you is the one thing the label is actually built around, someone licensed checking your glucose risk and your medications before anything ships [R4], and a real pharmacy standing behind what’s in the bottle instead of a warehouse. Credit to FormBlends for something a lot of sellers won’t say out loud: it states clearly that the FDA approval is for HIV lipodystrophy, and that broader use is off-label, rather than waving “FDA-approved” around like it covers everything.
One disclosure worth spelling out: brand Egrifta is an FDA-approved finished drug. Compounded tesamorelin is not. What a compliant telehealth setup adds on top of that compounding is the oversight, the clinician, the prescription, the licensed pharmacy, the follow-up, none of which a research vial ever includes. Given that tesamorelin’s effects build over weeks and the glucose issue is worth tracking over time, that follow-up isn’t cosmetic. Logging your dose and any symptoms, say with the FormBlends tracker app, gives a clinician something concrete to look at next time instead of your fuzzy memory of “I think I felt a bit off in week three.” The app logs doses and symptoms. It’s not a prescription and it’s not a checkout.
HealthRX: same logic, second place
HealthRX (healthrx.com) lands right behind FormBlends because it’s built on the same foundation: licensed clinical oversight first, supervised dispensing through actual pharmacy channels, not a mailed research chemical. If you’re picking between these two, it comes down to practical stuff, which one’s licensed in your state and whose intake process suits you.
The research-chemical sellers, reviewed honestly
If you’re still leaning toward the powder route, I won’t hand you a “best pick” among them, because neither of us can verify which one actually ships clean tesamorelin. Without independent, batch-level testing, that ranking simply doesn’t exist to give. What I can tell you is what they all have in common. Swiss Chems sells tesamorelin next to SARMs, several of which carry their own doping baggage, all under “research use only” labels. Pure Rawz runs a broad catalog of research peptides and SARMs with the same structure and the same disclaimer. Core Peptides is a US-based research-chemical retailer that may publish a seller-issued certificate of analysis, but that’s a document the company chose to write, not an FDA-verified guarantee of what’s actually in the vial. Amino Asylum sells it at aggressive prices in a wide research catalog, same “not for human consumption” language.
Every one of them shares the same structural gap: no clinician, no prescription, no glucose screening, no pharmacy standing behind the contents, and human use that’s legally gray at best. Buy at this tier and you’ve made yourself the quality-control department, on a drug whose own label assumes medical monitoring.
Bottom line
If your goal for tesamorelin is off-label, no path here makes that goal medically “approved,” full stop. What the evidence does tell you is that this is a real drug with a real blood-sugar concern and cardiovascular safety that isn’t fully established [R4], and that’s an argument for supervision, not a reason to skip it. The prescription route puts a clinician and a pharmacy between you and that risk. The research-chemical route puts a warning label between you and any recourse. My pick on the prescription side is FormBlends first, HealthRX second. On the research-chemical side, my honest advice is to reconsider whether you need to be on this path at all.
Questions I’d ask if I were you
Is tesamorelin FDA-approved for weight loss or anti-aging? No. It’s approved only for reducing excess abdominal fat in people with HIV-associated lipodystrophy, and the label says outright it isn’t indicated for weight loss [R4]. Using it for regular belly fat, anti-aging, or a GH boost is off-label. Legal if a clinician prescribes it, but not the same as the FDA signing off on that use.
Does the trial data actually apply to a healthy person who just wants a flatter stomach? Not directly, no. The 412-patient NEJM trial, the 806-patient pooled analysis, and the Lancet HIV liver-fat study all enrolled people with HIV-associated conditions [R1][R2][R3]. Real effects, sure, but they describe that specific population, so they don’t automatically carry over to someone outside it.
Why does tesamorelin require blood-sugar monitoring? Because it can push glucose the wrong way, and the approved label carries a standing instruction to watch for changes in glucose metabolism [R4]. That’s the core safeguard the drug is designed around, which is why a supervised path, where someone checks your diabetes risk before you get anything, matters more than saving a few bucks.
Is compounded tesamorelin the same thing as brand Egrifta? Same molecule, different regulatory status. Egrifta is an FDA-approved finished drug. Compounded tesamorelin isn’t an FDA-approved product. What a legitimate telehealth setup adds on top of the compounding is the oversight layer, a clinician, a prescription, a licensed pharmacy, follow-up, that a research vial simply doesn’t have.
Is a “research use only” vial safe to inject just because tesamorelin itself is approved? No, and this is the trap I keep flagging. The approval doesn’t extend to a powder from a chemical retailer. That “research use only” label is the legal cover the product is sold under, and nothing independent confirms the vial actually contains properly dosed tesamorelin. The trial data describes real, pharmaceutical-grade tesamorelin, not whatever’s in an unverified bottle. Buy from that tier and you’re the one doing quality control.
Is tesamorelin banned in competitive sport? Yes, named directly on the WADA 2026 Prohibited List under category S2 as a growth-hormone-releasing factor [R5]. Banned no matter how you got it, so a “research use only” sticker offers a tested athlete zero protection. Check the current list before going near it.
What tesamorelin is and how it works, in plain terms
Tesamorelin is a lab-made version of growth hormone-releasing hormone (GHRH), something your hypothalamus already makes. It works by telling your pituitary gland to produce and release more of your own growth hormone, rather than injecting synthetic GH straight into your system. That distinction matters because your pituitary still applies its normal feedback brakes, generally considered a safer hormonal profile than dosing GH directly.
Does the FDA approval cover everyone who wants it?
No. The FDA approved tesamorelin in 2010 as Egrifta for one specific job: reducing excess abdominal fat in HIV-positive adults with lipodystrophy. It doesn’t extend to general weight loss, anti-aging, or body-composition goals in otherwise healthy people. Anything outside that indication is off-label, meaning less regulatory scaffolding and more weight on the prescribing clinician’s judgment call.
Do you need to be asleep for it to work?
No. The advice to inject at night just mirrors your body’s natural GH pulse, which peaks early in sleep, and may line the extra stimulus up with your body’s own timing. Morning and evening injections both show activity in clinical use. Consistency matters more than the exact hour, so pick a time you can actually stick to.
Where does a compounding pharmacy fit versus raw peptide powder off a website?
A physician-supervised compounding pharmacy operates under state pharmacy board rules and USP quality standards, so what you get has been tested, labeled, and dispensed against an actual prescription. Raw peptide powder sold online as a “research chemical” has none of that accountability behind it, purity, dosing accuracy, and sterility are all unverified. The gap isn’t just paperwork. It’s the difference between knowing and guessing what you’re injecting.
References
- Tesamorelin reduced visceral adipose tissue by 15.2% (versus a 5.0% increase on placebo), lowered triglycerides by about 50 mg/dL, and raised IGF-1 by about 81% in a 26-week Phase 3 trial of 412 HIV patients. New England Journal of Medicine, 2007. https://pubmed.ncbi.nlm.nih.gov/18057338/
- Pooled analysis of two Phase 3 tesamorelin trials (806 HIV patients); visceral-fat reduction and lipid improvements maintained to 52 weeks. Journal of Clinical Endocrinology and Metabolism, 2010. https://pubmed.ncbi.nlm.nih.gov/20554713/
- Tesamorelin reduced liver fat in HIV patients with fatty liver disease; about 35% of treated patients reached a normal liver-fat fraction versus 4% on placebo. Lancet HIV, 2019.
- FDA-approved Egrifta (tesamorelin) prescribing information: indicated for reduction of excess abdominal fat in HIV-infected patients with lipodystrophy; 2 mg subcutaneous once daily; monitor for changes in glucose metabolism; long-term cardiovascular safety not established; not indicated for weight loss. U.S. Food and Drug Administration label (original 2010 approval).
- WADA 2026 Prohibited List: growth-hormone-releasing hormone analogues, including tesamorelin, are prohibited in sport under category S2. World Anti-Doping Agency, in force January 2026.